




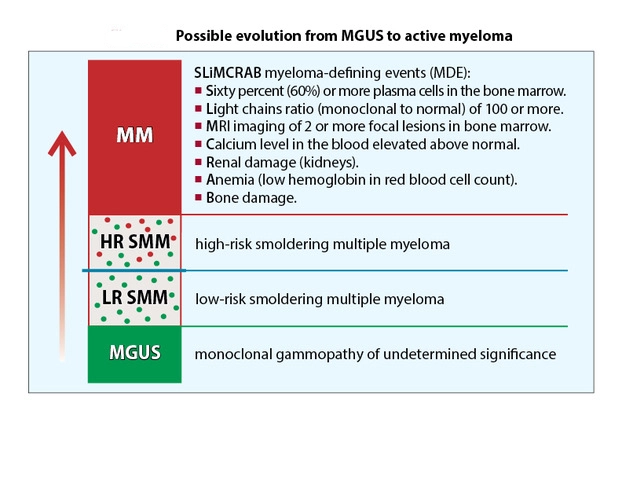
Multiple myeloma (MM) patients must undergo a careful diagnostic workup to stage their disease. Before developing active myeloma, patients pass through two earlier disease stages — monoclonal gammopathy of undetermined significance (MGUS) and smoldering multiple myeloma (SMM).
MGUS is the first stage of myeloma before symptoms are present. It's a benign precursor to multiple myeloma, and patients with MGUS may or may never develop active myeloma.
In some patients, MGUS may progress to SMM, which is also asymptomatic. SMM will eventually progress to active myeloma. In most cases, doctors will observe SMM patients without advising treatment until the condition progresses. However, some clinicians may recommend early intervention with high-risk SMM patients. This intervention would most likely be conducted through a clinical trial.
MM, or active myeloma, is a cancer of the plasma cells produced in the bone marrow. Unlike MGUS and SMM, it has symptoms ranging from bone pain to fatigue. Understanding how the disease progresses is vital to navigating a diagnosis.
Jump to a section:
- Table Defining MGUS, SMM, and Active Myeloma
- Understanding MGUS
- What’s Needed for an MGUS Diagnosis?
- Risk Progression of MGUS to Myeloma
- Understanding Smoldering Multiple Myeloma
- Diagnostic Criteria for SMM
- Mayo Clinic’s 2/20/20 Criteria
- When Might SMM Progress?
- Treatment for Smoldering Multiple Myeloma
- Clinical Trials for Smoldering Multiple Myeloma
- What Is Active Myeloma?
- Diagnosing Active Myeloma
- Quality of Life After Diagnosis
- Find Your Local Group
- What’s Next?
Table Defining MGUS, SMM, and Active Myeloma
| MGUS (benign) | SMM (pre-malignant) | Myeloma (malignant) | |
| Clonal plasma cells in bone marrow | <10% | 10%-60% | ≥10% |
| Presence of myeloma-defining events | no | no | yes |
| Likelihood of progression | ~1% per year | ~10% per year | not applicable |
| Management | observation only | observation, clinical trials, or treatment if high-risk SMM | treatment |
Understanding Monoclonal Gammopathy of Undetermined Significance
MGUS occurs when plasma cells secrete abnormal monoclonal proteins (M proteins) into the blood. If you have been diagnosed with or are suspected to have MGUS, see an experienced hematologist. A hematologist is a doctor who specializes in the problems of blood and bone marrow.
While MGUS is a benign condition, it can sometimes progress to smoldering multiple myeloma, a premalignant stage that requires careful monitoring by a healthcare professional.
Some facts about MGUS
- MGUS occurs in 3% to 5% of the population in the United States.
- This rate is higher for those who are 50 years of age or older.
- MGUS is the earliest disease state associated with the subsequent development of myeloma.
MGUS is typically asymptomatic, meaning that most individuals do not experience any noticeable symptoms related to the condition.
What Are the Types of MGUS?
This webpage discusses the plasma cell type of MGUS, which comprises 85% of all MGUS cases. Yet, MGUS can arise from either plasma cells or lymphoid cells, and these two types of MGUS are biologically different.
Plasma cell type MGUS
This type of MGUS can progress to become myeloma or a related disorder, including amyloidosis and light chain deposition disease (LCDD). Plasma cells develop from a type of white blood cell (WBC) called B cells (B lymphocytes) and are a key part of the immune system. In the normal immune response, B cells mature into plasma cells in the bone marrow. In bone marrow, plasma cells produce antibodies that attach to antigens that enter the body.
How Is MGUS Diagnosed?
MGUS is generally asymptomatic. It is usually discovered through laboratory testing performed during the evaluation of other conditions.
What Is the Significance of M-Proteins?
People with MGUS have relatively low levels of monoclonal protein (myeloma protein, M-protein) in their blood or urine. The amount of M-protein reflects the activity of abnormal plasma cells in the bone marrow.
Tests for M-Proteins
The laboratory tests used to measure the amount of M-protein include the following:
- serum protein electrophoresis (SPEP)
- urine protein electrophoresis (UPEP)
- serum free light chain (sFLC)
- urine free light chain (uFLC)
Your plasma cells can produce one of five classes (isotypes) of immunoglobulin:
- IgG
- IgA
- IgD
- IgE
- IgM
Immunofixation electrophoresis (IFE) is an immunologic test of the serum or urine. It is used to identify the exact heavy-chain and light-chain type of M-protein that is present.
An immunoglobulin light chain is the smaller of two units that make up an antibody. Two types of light chains are kappa and lambda. A light chain may be bound to a heavy chain by chemical bonds, or it may be unbound and "free" to enter the bloodstream. Free light chians that circulate in the blood are small enough to pass into the kidneys. There, these free light chains may be filtered into the urine or they may stick together and block the kidney's tubules.
What Happens After the Tests?
After MGUS is diagnosed, monitoring should be done every three to six months, including a complete blood count (CBC), SPEP/UPEP, and sFLC. If your M-protein remains stable and there are no other symptoms or health changes, your doctor can extend the time between follow-up testing. Be sure to report any change in your health to your doctor.
At the discretion of your doctor, additional testing may be performed, including bone marrow testing. A bone marrow biopsy is recommended if the patient has CRAB criteria:
- unexplained hypercalcemia
- kidney dysfunction
- anemia
- bone lesions
- or suspicion of amyloid light-chain (AL) amyloidosis.
What's Needed for an MGUS Diagnosis?
For an MGUS diagnosis, all of the following criteria must be met:
- Presence of M-protein in the serum < 3 g/dL,
- Presence of monoclonal plasma cells in the bone marrow < 10%, and
- Absence of CRAB criteria.
For a diagnosis of light chain MGUS, all of the following criteria must be met:
- Abnormal free light chain (FLC) ratio < 0.26 or > 1.65,
- Level of the appropriate involved light chain (increased kappa FLC in patients with a ratio > 1.65 and increased lambda FLC in patients with a ratio < 0.26),
- No immunoglobulin heavy chain expression on IFE,
- Absence of CRAB criteria,
- Presence of monoclonal plasma cells in the bone marrow < 10%, and
- Presence of M-protein in the urine based on a 24-hour collection < 500 mg.
If your test results indicate myeloma or another protein disorder, additional testing will be performed to establish a diagnosis. These tests will likely include the following:
- lactate dehydrogenase (LDH)
- beta-2 microglobulin (β2M), and
- C-reactive protein (CRP).
If the test results are within normal ranges, you will be tested again in six months with SPEP and CBC. Then, you will also be tested annually for life or until changes occur.
What Is the Risk Progression of MGUS to Myeloma?
Progression from MGUS to active myeloma occurs at the low rate of only 1% per year. Only 20% of people diagnosed with MGUS will ever develop myeloma. It is not yet known what triggers progression. Researchers are working to gain a better understanding of biologic events that take place when MGUS develops into myeloma.
The IMF International Myeloma Working Group (IMWG) has established the following risk factors for MGUS progressing to myeloma:
- M-protein level is more than 1.5 g/dL (can also be written as 15 g/L),
- M-protein type is IgA or IgM, and
- Abnormal FLC ratio of kappa to lambda FLCs.
Risk of progression from MGUS to active myeloma:
- Low-intermediate-risk MGUS has one of the risk factors.
- High-intermediate-risk MGUS has two of the risk factors.
- High-risk MGUS has all three of the risk factors.
If you are diagnosed with intermediate-risk or high-risk MGUS during your baseline testing, you should also have a bone marrow aspiration and bone marrow biopsy. The same bone marrow sample that is obtained should also be used for cytogenetic studies. Visit Tests to assess monoclonal protein to learn about the tests used to identify and quantify M-protein.
How Should MGUS Be Managed?
At this time, there is no treatment for MGUS that are approved by the U.S. Food and Drug Administration (FDA). Monitoring MGUS as described above can determine if any progression is occurring and if any additional testing is required. The risk of progression is 1% per year. The majority of MGUS patients are monitored without the need for additional medical attention for many years.
MGUS and the IMF's iStopMM Study
Launched in November 2016, iStopMM® (Iceland Screens Treats or Prevents Multiple Myeloma) is the largest-ever population-based screening study for MGUS, SMM, and myeloma. The iStopMM study invited the approximately 140,000 residents of Iceland who are over age 40 to be screened for the presence of M-protein in the serum or urine. More than half of the invited population volunteered to take part in the iStopMM study.
The iStopMM study is monitoring people with MGUS in order to better understand disease biology, identify the genes that drive disease progression, and determine who may benefit from early intervention.
The many outcomes from the iStopMM study will benefit not only Iceland but the myeloma community around the world. iStopMM is supported by the IMF Black Swan Research Initiative® (BSRI®).
Understanding Smoldering Multiple Myeloma
Smoldering multiple myeloma (SMM) is an asymptomatic (no signs or symptoms) precursor state of active myeloma. Similar to MGUS, M-protein is present in people with SMM, but the amount of M-protein is greater with SMM than with MGUS. Between 10% and 60% myeloma cells are present in the bone marrow of people with SMM.
SMM and the IMF's iStopMM Study
An important early finding from the iStopMM study was that the prevalence of SMM is higher than expected:
- 0.53% in persons 40 years or older
- 0.67% in men
- 0.39% in women, with the prevalence increasing with age
This finding enhances the potential value of screening in that early interventions can be offered with hopes of improved outcomes.
How Is Smoldering Multiple Myeloma Diagnosed?
Smoldering multiple myeloma may be diagnosed in these scenarios:
- When a person with MGUS is being observed by their healthcare team,
- In the course of a routine exam, or
- When an individual seeks or receives care for another condition.
What Are the Diagnostic Criteria for Smoldering Multiple Myeloma?
For SMM, the diagnostic process includes the following tests:
- CBC
- chemistries (measurement of calcium and creatinine values)
- SPEP
- sFLC
At the time of a SMM diagnosis and within two to three months after the diagnosis, a 24-hour urine collection for electrophoresis and immunofixation should be performed. A baseline bone marrow biopsy and imaging should also be performed.
For a diagnosis of SMM, both of the following criteria must be met:
- Presence of M-protein in the serum (IgG or IgA) ≥ 3 g/dL, or urinary M-protein ≥ 500 mg per 24-hour collection, and/or presence of monoclonal plasma cells in the bone marrow 10%–60%, and
- Absence of myeloma-defining events (MDE) or amyloidosis.
Myeloma-defining events (MDE) include the following:
- Presence of CRAB criteria,
- Presence of monoclonal plasma cells in the bone marrow ≥ 60%,
- Ratio of involved-to-uninvolved serum FLC ≥ 100 (involved FLC level must be ≥ 100 mg/L and urine M-protein level must be at least 200 mg per 24-hour collection on UPEP), and
- One or more focal lesions on magnetic resonance imaging (MRI) studies.
Once SMM is diagnosed, current clinical guidelines recommend stratification to determine the risk of progression to active myeloma, as well as lifelong monitoring for progression.
The Mayo Clinic’s 2/20/20 Criteria
In 2018, the Mayo Clinic published the 2/20/20 criteria. These criteria are based on patients who had none, one, or two to three of the risk factors that were most associated with a short time to progression from SMM to active myeloma:
- Serum M-protein > 2 g/dL,
- Bone marrow plasma cell (BMPC) infiltration > 20%, and/or
- Ratio of involved-to-uninvolved serum FLC > 20.
Once SMM is diagnosed, current clinical guidelines recommend stratification to determine the chance of progression to myeloma and lifelong monitoring for progression.
The current understanding of the biology and behavior of SMM enables doctors to avoid treating patients who do not need to be treated, but to intervene promptly if a patient is at a high risk of advancement to myeloma.
The doctor’s experience and judgment are crucial to differentiating MGUS from SMM and from active myeloma. A primary consultation or second opinion with a myeloma expert is highly recommended.
Note: Of the 193 participants in the iStopMM study who were diagnosed with SMM, the median age was 70 years (range 44–92) and 60% were males.
Monitoring SMM with Imaging Studies
The doctor monitoring your SMM will discuss the following imaging studies with you:
- Whole-body low-dose CT (WBLCT) does not require the use of contrast agents and uses much less radiation than conventional CT. It is considered the standard of care to detect and document early bone disease.
- Magnetic resonance imaging (MRI) of the spine and pelvis are highly recommended because these sensitive studies are better able to predict for more rapid progression to active myeloma.
- Positron emission tomography (PET) imaging scan be combined with WLBDCT or MRI to reveal "hotspots" areas in the body where myeloma cells can accumulate and cause damage.
Skeletal X-rays are no longer the standard of care in the diagnostic process of SMM because they only pick up bone lesions after approximately 30% of the cancellous bone has been destroyed.
How Are Patients with Smoldering Multiple Myeloma Monitored?
Patients with SMM are monitored more frequently than patients with MGUS because the risk of progression to active myeloma is higher.
- If you have been diagnosed with SMM, you must be carefully evaluated by a hematologist-oncologist every four to six months for the first year.
- If your SMM remains stable after a year, the evaluation can be lengthened to every 6 to 12 months based on your SMM status and your doctor’s judgment.
When Might SMM Progress to Active Myeloma?
Ongoing research is being conducted to identify the risk factors for progressing from SMM to active myeloma. A system of precise criteria does not exist now. However, the average risk progression from SMM to active myeloma is 10% per year.
In 2014, The Lancet published the IMWG updated criteria for the diagnosis of myeloma. SMM patients with 80% or greater risk of progression to myeloma within 2 years were defined as having early active myeloma. To help prevent the development of end-organ damage, a patient should be treated for myeloma if any of the myeloma-defining events (MDE) are present.
In 2018, Blood Cancer Journal published a statistical analysis of variables among patients with SMM at Mayo Clinic in Rochester, Minnesota. Further refinements to the 2/20/20 criteria were made with the addition of the following two high-risk factors:
- chromosomal abnormality +1q (a gain of chromosome 1q),
- chromosomal abnormality del13q (a deletion of chromosome 13q).
If one or both of these abnormalities are found by fluorescence in situ hybridization (FISH) testing of myeloma cells, the risk of disease progression is increased.
In 2020, Blood Cancer Journal published the IMWG risk stratification model for SMM that can be applied across the globe using easily available data.
Dr. María-Victoria Mateos and colleagues assembled an international cohort of 1,996 patients with SMM who met the revised IMWG criteria. Patients with ≥ 80% risk of progression at 2 years were excluded because they are considered to have active myeloma by current definition.
Factors Representing a High Chance of Progression
Three independent factors were identified predicting high-risk SMM (HR SMM) progression to active myeloma at 2 years based on the 2/20/20 criteria. This translates into 3 categories with an increasing 2-year progression risk:
- 6% for low-risk patients with no risk factors,
- 18% for intermediate-risk patients who have 1 factor, and
- 44% for high-risk patients who have 2 or more factors.
In addition, presence of chromosomal abnormalities t(4;14), t(14;16), +1q, and/or del13q allowed for further separation into the following 4 groups:
- Low-risk SMM patients had no cytogenetic abnormalities. Low risk of progression to active myeloma.
- Low intermediate-risk SMM patients with 1 cytogenetic abnormality had the progression risk at 2 years of 23%.
- Intermediate-risk SMM patients with 2 cytogenetic abnormalities had the progression risk at 2 years of 46%.
- High-risk SMM (HR SMM) patients with 3 or more cytogenetic abnormalities had the progression risk at 2 years of 63%.
What Is the Treatment for Smoldering Multiple Myeloma?
Typically, SMM is not treated. Yet, based on the risk of progression of a patient's SMM, some of these patients may have available treatment options.
As discussed earlier, SMM patients are either low-risk, low-intermediate-risk, intermediate-risk, or high-risk. For the first three risk categories mentioned, no treatment is recommended, but rather, continuous observation.
FDA approves first treatment for high-risk smoldering multiple myeloma
In November 2025, the FDA granted its first approval of a treatment for adult patients with high-risk smoldering multiple myeloma (HR-SMM). The FDA approval of Darzalex Faspro® (daratumumab + hyaluronidase-fihj) monotherapy is based on data from the AQUILA clinical trial, which compared treatment with Darzalex for 3 years vs. active monitoring (observation) in 390 patients with HR-SMM.
Patients randomized to the treatment arm of the study received 1,800 mg of daratumumab and 30,000 units of hyaluronidase-fihj as a subcutaneous (SQ) injection under the skin once-weekly for 2 cycles (1 cycle = 4 weeks) and then every other week for 4 cycles, and then every 4 weeks until 39 Cycles of treatment or up to 36 months or until diagnosis to myeloma or unacceptable toxicity. For more information about this drug and its poten tial side effects, read the IMF’s publication Understanding DARZALEX® (daratumumab) and DARZALEX FASPRO® (daratumumab + hyaluronidase-fihj).
Darzalex Faspro is approved for patients with HR-SMM; it is not approved for other risk categories of SMM.
What Are Some Clinical Trials for Smoldering Multiple Myeloma?
A clinical trial is a medical research study with people who volunteer to test scientific approaches for preventing, detecting, diagnosing, or treating cancer, or to answer scientific questions. A clinical trial is launched only after laboratory studies have demonstrated the potential of a new treatment or procedure to be more effective or less harmful than existing methods. The goal of clinical trials is to improve patient care. Many studies are evaluating treatment choices in SMM. Noted below are three key studies that produced important data about the role of treatment in SMM.
The LINKER-SMM1 clinical trial
Preliminary results presented at the 2025 International Myeloma Society (IMS) annual meeting on the use of Lynozyfic™ (linvoseltamab) monotherapy for people with HR-SMM demonstrated a response rate of 100% in the group of 20 study patients. Lynozyfic is a bispecific antibody; you can learn about it in the IMF’s publication Understanding LYNOZYFIC™ (linvoseltamab-gcpt).
The CAR-PRISM clinical trial
Carvykti® (ciltacabtagene autoleucel) is a chimeric antigen receptor (CAR) T-cell therapy currently approved by the FDA for patients with relapsed or refractory multiple myeloma (RRMM), and this approach is delivering deep and durable responses for many patients. The objectives of the CAR-PRISM study of Carvykti in HR-SMM are to determine safety and assess efficacy.
Six patients with HR-SMM have been treated, with a median follow-up of 6 months (60 days to 1 year). All patients achieved MRD-negativity at 10-6 by day 28 and MRD-negativity was sustained in all patients to date of the ASH presentation without any evidence of disease progression. The overall response rate (ORR) is 100%, with a complete response (CR) rate of 50% and responses deepening over time. Long-term follow up is required to determine if the study responses will be sustained. For more information, read the IMF’s publication Understanding CARVYKTI® (ciltacabtagene autoleucel).
The ASCENT clinical trial
The ASCENT clinical trial was designed as an attempt to cure patients with HR-SMM. While the answer to this question can come only after years of follow-up, patients in the study arm of combination therapy with Darzalex the proteasome inhibitor Kyprolis® (carfilzomib) the immunomodulatory agent Revlimid® (lenalidomide), and the steroid dexamethasone [DKRd] achieved high rates of deep and durable responses, including high rates of sustained MRD-negativity. Treatment was given for a fixed duration of 2 years and was well-tolerated. The responses appear durable, with the 3-year progression-free survival (PFS) rate of 90%.
Finding a study to match your needs
A clinical trial may give you access to treatment that is not yet available outside of a study.
If you have SMM and are interested in participating in a clinical trial, it is essential to discuss with your doctor all the potential risks and benefits in your particular case, including the physical and psychological aspects of treatment as opposed to observation.
To help with personalized support for exploring clinical trial options across the U.S., the IMF has partnered with SparkCures. Visit myeloma.org/sparkcures or contact the IMF InfoLine for more information.
The U.S. government maintains the website clinicaltrials.gov, an online database of thousands of research studies from around the world. You may wish to also explore this resource. However, the U.S. government does not review or approve the safety and science of all the studies listed on this website.
For more information about what’s involved in study participation, read the IMF’s publication Understanding Clinical Trials in Myeloma.
What Is Active Myeloma?
All patients who develop active myeloma have previously had MGUS followed by SMM. A patient with SMM may remain at the "smoldering" stage for years without progressing to active myeloma. However, if you are at risk of progressing to active disease or if you have already been diagnosed with myeloma, this is the time to seek an opinion (or a second opinion) from a myeloma specialist.
Myeloma is a cancer of the bone marrow plasma cells, which are white blood cells that make antibodies. According to the National Cancer Institute SEER Program, myeloma represents only 1.8% of all new cases of cancer diagnosed in the U.S. in 2024. A local hematologist or oncologist might see a few myeloma patients or none at all.
Myeloma specialists at large "high-volume" treatment centers or academic institutions treat hundreds of myeloma patients, conduct clinical trials with new drugs and new combination therapies, and develop the expertise needed to help you make good decisions about your care.
Diagnosing Active Myeloma
A diagnosis of active myeloma is made when the patient experiences the following:
- 10% or more clonal plasma cells in bone marrow, and
- at least one myeloma-defining event (MDE).
Myeloma is a highly individual disease. Often, it is slow-moving. Sometimes, it can be very aggressive. The urgency of treatment depends upon the exact problems faced by an individual patient. An experienced myeloma specialist can tailor a treatment approach best suited to your specific situation, as well as anticipate and prevent or mitigate treatment-related problems.
Many highly effective therapies are approved for treating myeloma by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), and by other regulatory agencies. New approvals are expanding treatment options, and the rate of development of new drugs continues to accelerate.
Quality of Life After Diagnosis
Many patients with myeloma lead full and productive lives for years, even decades, after diagnosis. Survival and quality of life of myeloma patients are improving steadily. Learning about myeloma and understanding how it is treated can help patients and their loved ones reduce anxiety and gain a sense of control. Overall, it makes it easier to come to terms with the diagnosis.
Medical Problems Related to Myeloma
Find Your Local Group
The International Myeloma Foundation has various support groups to assist you on your journey. Find a local group or join the online community today.
What’s Next?
With advancements in medicine, thousands of people have gone on to live thriving, abundant, and full lives after having been diagnosed with active myeloma. The most important step you can take next is staying informed about MM and what you can expect based on the type you have.
By understanding the kind of myeloma you have, you and your healthcare team can assess how your disease may progress and how it should be treated.

Understanding the type of myeloma you have will help you and your healthcare team assess how your disease may progress and how it should be treated.












The International Myeloma Foundation medical and editorial content team
Comprised of leading medical researchers, hematologists, oncologists, oncology-certified nurses, medical editors, and medical journalists, our team has extensive knowledge of the multiple myeloma treatment and care landscape.
Additionally, the content on this page is medically reviewed by myeloma physicians and healthcare professionals.
Last Medical Content Review: March 6, 2026