




International Staging System for Multiple Myeloma
Developed in 2005 by the International Myeloma Working Group (IMWG), the ISS was built on clinical and laboratory data from 10,750 previously untreated myeloma patients across 17 institutions in North America, Europe, and Asia. It uses two readily available blood tests to classify patients into three stages. The following are those two blood tests:
- Serum β2 microglobulin (Sβ2M): A small protein found on most cells that circulates in blood and urine. Elevated levels may indicate disease activity, though it is a nonspecific marker also associated with lymphoma and kidney issues.
- Serum albumin: A protein made by the liver that helps maintain fluid in the bloodstream. Low levels can signal liver disease, chronic inflammation, or kidney problems. Importantly, low albumin also affects total calcium measurements, since albumin binds calcium.
ISS Stages and Criteria
The following table indicates the stages and correlating measurements according to ISS:
| Stage | VALUES (β2M = Serum β2 microglobulin; ALB = serum albumin |
| I | Sβ2M < 3.5 mg/L; serum albumin ≥ 3.5 g/dL |
| II | Sβ2M < 3.5 mg/L; serum albumin < 3.5 g/dL; or β2M 3.5 to 5.5 mg/L, irrespective of serum albumin |
| III | Sβ2M > 5.5 mg/L |
Revised International Staging System for Multiple Myeloma
Published by the IMWG in August 2015, the R-ISS expanded upon the ISS by incorporating two additional prognostic markers assessed from bone marrow samples taken at the time of diagnosis:
- Lactate dehydrogenase (LDH): An enzyme whose elevated levels can reflect more aggressive disease activity.
- Chromosomal abnormalities (cytogenetic abnormalities): Detected by fluorescence in situ hybridization (FISH), a technique that uses fluorescent chemical probes to bind to specific DNA sequences on chromosomes, revealing structural differences. The high-risk chromosomal abnormalities assessed are del(17p), t(4;14), and t(14;16).
R-ISS Myeloma Stages and Criteria
These revised indicators form a more powerful prognostic index:
| Stage | Criteria |
| I | Sβ2M < 3.5 mg/l Serum albumin ≥ 3.5 g/dl Standard-risk chromosomal abnormalities (CA) by iFISH Normal LDH |
| II | Not R-ISS stage I or III |
| III | Sβ2M ≥ 5.5 mg/L and either High-risk CA by FISH OR High LDH |
While the R-ISS incorporates genetic risk markers, it does not always reflect real-world outcomes or current treatment standards — such as triplet and quadruplet drug combinations. This limitation motivated further refinement of the classification framework.
The IMWG-IMS Classification (2025)
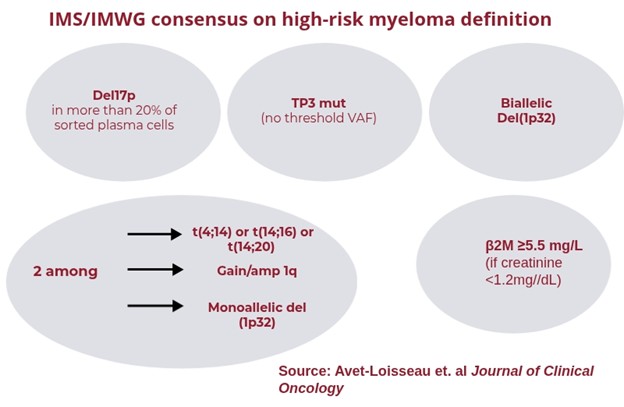
In June 2025, the IMWG and the International Myeloma Society (IMS) jointly published a new consensus classification of high-risk multiple myeloma. This framework incorporates the most recent research data and advances in treatment, offering a more modern and biologically informed approach to risk stratification.
Its primary purpose is to guide clinical decisions around treatment intensity, treatment duration, and clinical trial enrollment. Patients are divided into two groups: Standard-Risk and High-Risk.
IMWG-IMS Classification Criteria
There are five ways of being defined as high-risk, as outlined by this diagram:
Understanding Treatment Response
While staging and risk stratification guide initial treatment decisions, monitoring treatment response is equally important for managing myeloma over time.
After beginning treatment (induction therapy), your doctor will assess how well the myeloma is responding by measuring monoclonal protein levels. Response depth is categorized as follows:
Most patients achieve deep remission with modern combination therapies. Remission is often maintained long-term with continuous or maintenance therapy. However, because myeloma is a relapsing disease, most patients will eventually experience disease progression requiring new treatment approaches.
Other Factors That Influence Outcomes
Staging and risk stratification are important clinical tools, but several additional factors can influence a patient's prognosis and treatment options:
- Age: The most common age range at diagnosis is 65–74. Frailty and co-morbidities in older patients may limit access to certain treatment options and reduce tolerance for side effects.
- Kidney function: Healthier kidneys and lower creatinine levels are associated with better outcomes. Monoclonal immunoglobulin can impair kidney function, making it harder for the kidneys to filter creatinine from the blood. Elevated creatinine can worsen prognosis and restrict treatment choices.
- Overall health: Existing conditions such as diabetes or heart disease affect both myeloma outcomes and tolerance to treatment.
- Response to therapy: Myeloma that does not respond to treatment or only responds for a short period of time — even in the absence of high-risk chromosomal abnormalities — indicates "functional" high-risk disease and carries a poor prognosis.
- Extramedullary disease (EMD) - although myeloma originates in the bone marrow, it can grow in other tissues and is termed “extramedullary” (meaning outside the marrow). This can be associated with more aggressive myeloma
- Plasma Cell Leukemia (PCL) - myeloma cells (cancerous plasma cells) are typically found in the bone marrow. Yet, in some cases, they can be found in the peripheral blood. This is also associated with a more aggressive form of myeloma.
An Important Note on Interpretation
The presence of high-risk features does not automatically mean a patient's myeloma will behave aggressively. Some patients with high-risk classifications experience less aggressive disease, while some patients with standard-risk classifications may face more aggressive disease courses. These systems are tools to guide clinical thinking — not deterministic predictions of individual outcomes.
Get More Information From the International Myeloma Foundation
If you are looking for resources and support, you can trust the IMF. We publish articles and videos to ensure you have as much information as possible, and we can help you find a local support group. For support resources, patients with high-risk multiple myeloma can contact the IMF's virtual high-risk multiple myeloma support group at [email protected].
What's Next?

If you are a newly diagnosed myeloma patient, learn when and if to begin treatment. Also, if you have undergone an induction therapy, learn about maintenance therapy and other new interventions.

The International Myeloma Foundation medical and editorial content team
Comprised of leading medical researchers, hematologists, oncologists, oncology-certified nurses, medical editors, and medical journalists, our team has extensive knowledge of the multiple myeloma treatment and care landscape.
Additionally, the content on this page is medically reviewed by myeloma physicians and healthcare professionals.
Last Medical Content Review: May 12, 2026