




Induction therapy followed by autologous stem cell transplantation (ASCT) before maintenance is the standard of care for transplant eligible NDMM patients. The addition of daratumumab to bortezomib, thalidomide, and dexamethasone (VTD) improved response rates and reduced the risk of progression or death compared to VTD alone (Moreau et al, Lancet 2019). Other quadruplet combinations such as carfilzomib, lenalidomide, dexamethasone and daratumumab have also been evaluated, showing high response rates and high levels of MRD negativity (Landgren et al, JAMA Oncol 2021), which seems particularly suitable to high-risk patients. The replacement of bortezomib with ixazomib in an all-oral combination with lenalidomide and dexamethasone (IRD) has been demonstrated to be safe, convenient, and effective in induction and consolidation before and after ASCT (Moreau et al, Blood 2017). The more progressive response kinetics and the very safe profile of ixazomib led to consider daratumumab plus IRD (D-IRD) extended induction and consolidation in standard-risk NDMM patients. We evaluated its safety and efficacy before and after ASCT followed by lenalidomide maintenance as frontline therapy for patients with standard-risk NDMM younger than 66 years (NCT03669445).
Conclusion
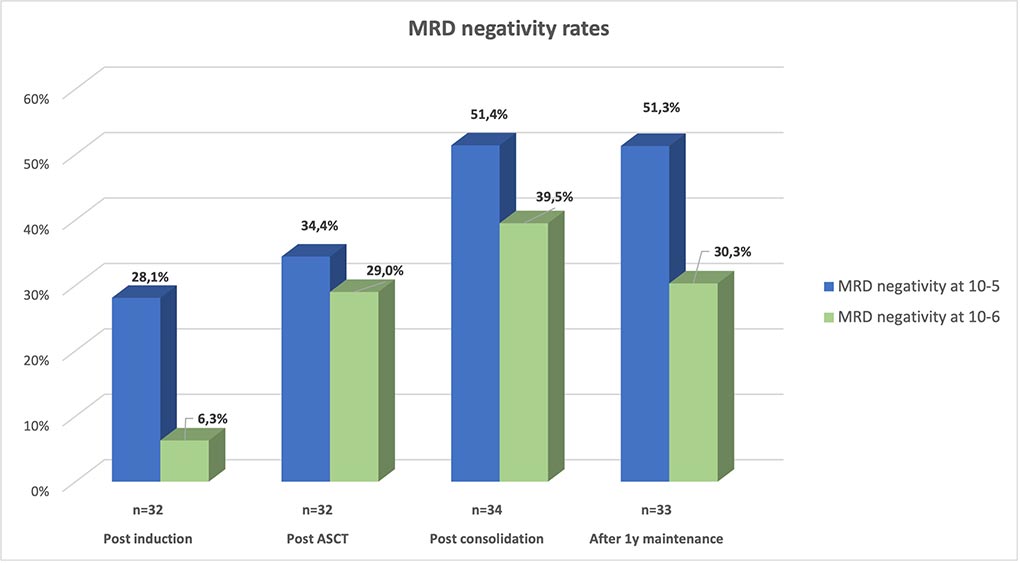
D-IRD as extended induction prior to, and as consolidation following ASCT was safe and allows gradually deepening responses in standard-risk MM, with 39.5% of patients with MRD negativity at 10-6 after consolidation, 2-year PFS at 95.2% and 2-year OS at 100%. MRD-negativity rates are lower than those obtained with D-VTD or D-KRD; more follow-up is needed to confirm PFS and OS data.
ASH 2021: Abstract 464
