





2024 ASCO and EHA Meetings Feature Four Phase III Clinical Trials and More!
By Dr. Joseph Mikhael, IMF Chief Medical Officer
Two very important annual medical meetings are held every spring, back-to-back, by the American Society of Clinical Oncology (ASCO) and the European Hematology Association (EHA). The 2024 annual meetings did not disappoint! During my more than 20 years working in myeloma, I don’t recall ever seeing FOUR large phase III clinical trials reporting their first data at ASCO and EHA. This speaks to the incredible progress made in myeloma over the past year.
It is my pleasure to summarize for you these four studies as well as several other abstracts presented at ASCO and/or EHA in five major areas.
Newly diagnosed multiple myeloma (NDMM)
Two of the phase III clinical trials presented were designed to evaluate the benefit of a quadruplet (4-drug) combination therapy in patients with NDMM who did not intend to proceed to an autologous stem cell transplant (ASCT).
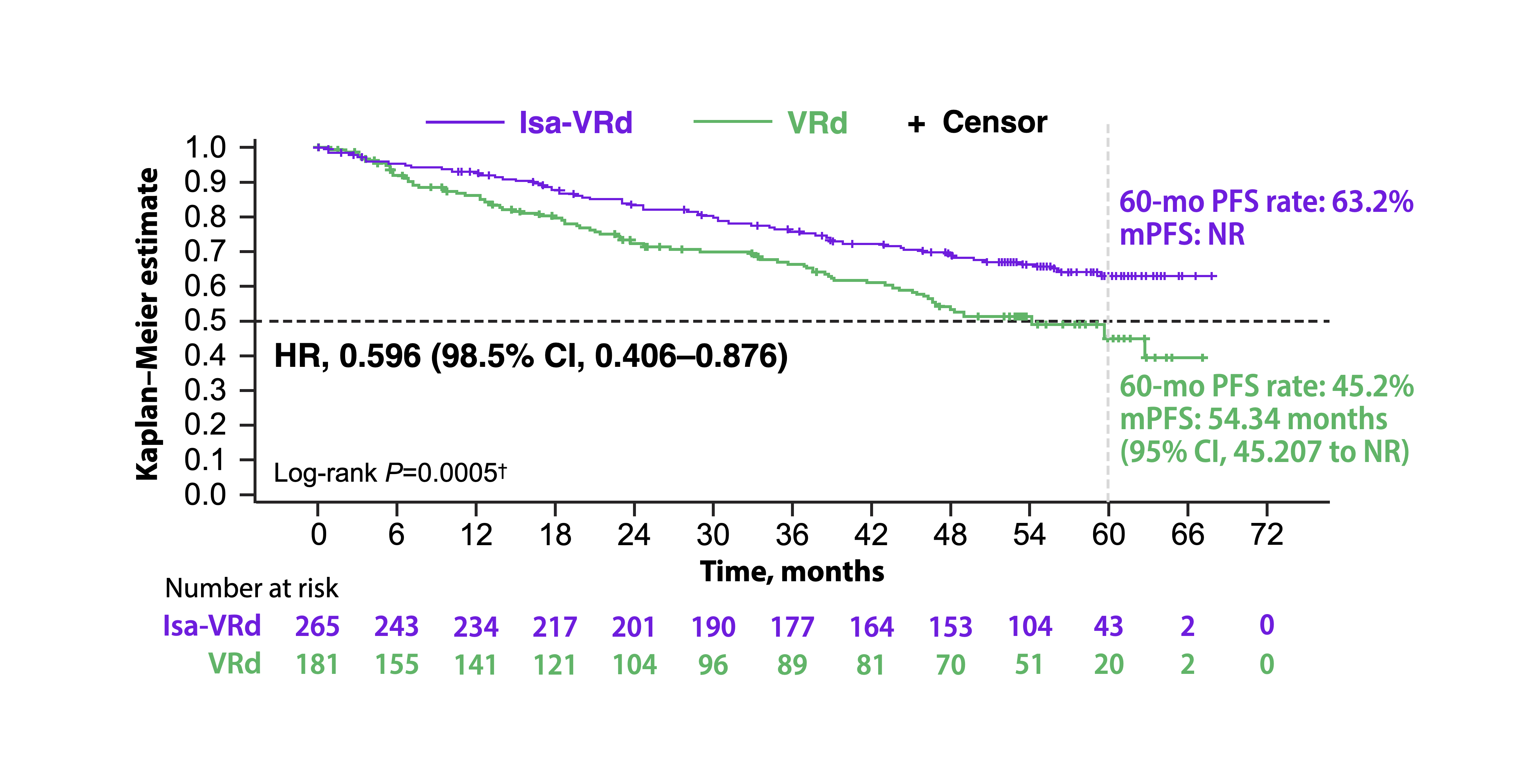
ASCO abstract #7500 IMROZ clinical trial (Facon) of Sarclisa® (isatuximab) in combination with Velcade® (bortezomib) + Revlimid® (lenalidomide) + dexamethasone [Isa-VRd] was compared to the triplet (3-drug) therapy with VRd. An impressive improvement in progression free survival (PFS) was demonstrated in the Isa-VRd arm, with 63% of study patients still in remission at 4 years vs. 45% of patients in the VRd arm.
ASCO abstract #7501 BENEFIT clinical trial (Leleu) compared Isa-VRd to Sarclisa + Revlimid + dexamethasone [Isa-Rd]. Interestingly, the primary endpoint in this study was not PFS but depth of response (DpR) as measured by minimal residual disease (MRD). The quadruplet of Isa-VRd demonstrated an impressive MRD negativity rate of 18 months. The Velcade in this trial was given weekly for one year, then every other week for 6 additional months.
Previously, at the December 2023 meeting of the American Society of Hematology (ASH), the PERSEUS clinical trial of quadruplet therapy with Darzalex® (dara tumumab) in combination with VRd [D-VRd] was shown to be superior to the triplet therapy with VRd in myeloma patients who were intending to proceed to ASCT.
Takeaway: Both IMROZ and BENEFIT studies demonstrate that in patients (under the age of 80) who do not intend to proceed to transplant, Isa-VRd is both feasible and effective, with deep and durable responses that will clearly move us to greater use of 4-drug combinations in this patient population. We still have to sort out the optimal dosing strategy for VRd, as we tend to use a “VRd-lite” approach in these patients, with less frequent administration of Velcade, lower doses of Revlimid, and more rapid dose-tapering of dexamethasone.
Early-line relapsed myeloma
There have been many important clinical trials that have guided our use of therapies when myeloma relapses. We are learning that it is particularly important to choose the individual patient’s optimal therapy early on in the myeloma disease course, that is if the therapy is accessible, rather than “saving it for later.”
In April 2024, the FDA expanded the approval of Carvykti® (ciltacabtagene autoleucel or “cilta-cel” for short) CAR T-cell therapy for the treatment of patients with relapsed refractory multiple myeloma (RRMM) who have received at least 1 prior line of therapy; this was based on data from the CARTITUDE-4 clinical trial. One day earlier, the FDA expanded its approval of Abecma® (idecabtagene vicleucel or “ide-cel” for short) for the treatment of RRMM after 2 or more prior lines of therapy; this was based on data from the KarMMa-3 clinical trial.
At ASCO and EHA, it was particularly encouraging to see data from studies with patients who have “functional” high-risk multiple myeloma (HRMM) – those who relapsed within 18 months of their initial response – and how CAR T-cell therapy can benefit them. For more information, read ASCO abstract #7504 CARTITUDE-4 (Costa) and the EHA abstract #S208 KarMMa-2 (Leleu)
In addition, two important phase III clinical trials with the antibody-drug conjugate (ADC) Blenrep® (belantamab-mafodotin), which was approved by the FDA for myeloma in 2020 but withdrawn from the market in the U.S. when the confirmatory phase III clinical trial was not positive. However, we now have two clinical trials that clearly show the benefit of Blenrep in early-line relapse.
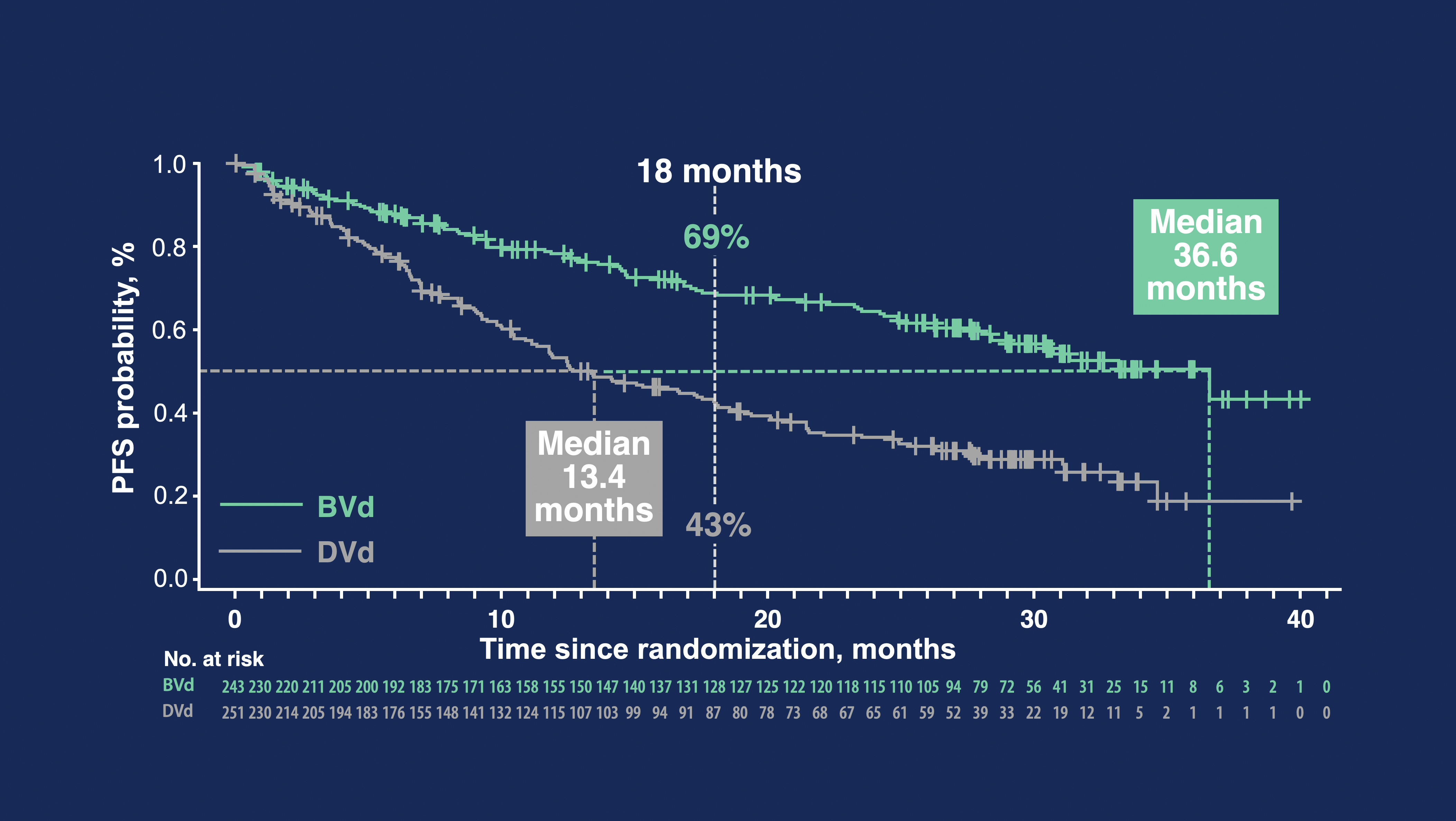
ASCO abstract #7503 DREAMM-7 (Mateos) of Blenrep in combination with Velcade + dexamethasone [BVd] vs. Darzalex in combination with Velcade + dexamethasone [DVd] demonstrated the median PFS (mPFS) for the BVd arm was an impressive 36 months vs. 14 months for the DVd arm. There was even a trend to an overall survival (OS) advantage in the Blenrep arm.
ASCO abstract #LBA103 DREAMM-8 (Trudel) of Blenrep added to Pomalyst® (pomalidomide) + dexamethasone [BPd] vs. Velcade + Pomalyst + dexamethasone [VPd] demonstrated a significantly longer median PFS in the Blenrep arm, which had not been reached at the time of presentation vs. PFS of 13 months in the VPd arm. Blenrep was added to Pomalyst® (pomalidomide) + dexamethasone [Pd] vs. Velcade + Pomalyst + dexamethasone [VPd]. The median PFS was significantly longer in the Blenrep arm and it had not yet been reached at the time of presentation vs. PFS of 13 months in the Velcade arm. At one year, 71% of patients in the Blenrep arm were still in remission vs. 51% in the Velcade arm. There were still a considerable number of patients who experienced eye symptoms like blurriness of vision, although it could be reversed with dose frequency reductions.
Takeaway: More CAR T-cell therapy will likely be used in early relapse, especially in patients whose myeloma relapses quickly after initial therapy. Also, we also expect to have Blenrep back in the clinic over the next year, as it is an easily delivered and highly effective treatment. However, we have more work to do on the optimal dosing of Blenrep to minimize the side effects.
CAR T-cell therapy
It was very exciting to see a whole series of new CAR T-cell therapies being developed. Although these are not yet ready to be used in the clinic, they have many features that would make them very attractive. “Fast” CARs feature a reduced manufacturing time so patients have a shorter wait for their T cells to be returned to them. Other features include lower risk of cytokine release syndrome (CRS) and other neurological side effects.
Takeaway: A newer generation of CAR T-cell therapies may result in even more effective outcomes with fewer side effects.
Bispecific antibodies
Bispecific antibodies have become an important part of late-line relapse therapy in myeloma. We have three FDA-approved agents in Tecvayli® (teclistamab-cqyv), Talvey® (talquetamab-tgvs), and Elrexfio® (elranatamab-bcmm). Updates to the original clinical trials were presented at both ASCO and EHA with encouraging results of ongoing response, even with less frequent dosing. It is becoming common practice to increase the interval between doses for all three bispecifics, from weekly to every other week or monthly. Several clinical trials are evaluating ways to provide bispecifics more easily and safely.
ASCO abstract #7517 (van de Donk) showed a dramatic drop in CRS from 72% to 25% with the use of prophylactic tocilizumab in patients treated with Tecvayli. There are many more new bispecific antibodies on the way, bringing the promise of reducing side effects (linvoseltamab), leveraging a new target of FcRH5 (cevostamab), or a treatment interval of every 4 weeks with no step-up dosing (ABBV-383).
Takeaway: New therapies in myeloma go through an “evolution” to make them more effective with lesser side effects. In addition, we will likely see an emphasis on more outpatient management, reducing dose intensity, and even stopping therapy at a defined period.
Sequencing of immunotherapies
Newer myeloma therapies like CAR T-cell therapies and bispecific antibodies raise the issue of the order in which they should be given. Several ASCO and EHA abstracts presented real-world data sets to sequence treatments of relapsing myeloma. At this time, there isn’t a “perfect” sequence, but certain themes have emerged.
The BCMA target on the surface of the myeloma cell that we use for CAR T-cell therapy and for two of the bispecifics (Tecvayli and Elrexfio) is not easily lost when treatment is given. The target can likely be leveraged more than once, going from one treatment to another, but the order is important. It may be preferable to go from CAR T to a bispecific, allowing a “break” for T cells between treatments. Lastly, short duration of response to one modality may encourage using a different target or approach, like switching to the GPRC5D target with Talvey.
Takeaway: As researchers continue to explore optimal sequencing of myeloma therapies, this topic should be part of the shared decision-making discussion that patients have with their healthcare team.
These are truly remarkable times in myeloma as we gain knowledge about the optimal use of the expanding array of effective tools to tackle this disease. I encourage you to visit myeloma.org/webcasts/ASCO-EHA to view IMF videos with myeloma key opinion leaders (KOLs) from ASCO and EHA.
To stay in the know about the key developments in the field of myeloma, sign up at subscribe.myeloma.org for our quarterly journal Myeloma Today and weekly e-newsletter Myeloma Minute, and contact the IMF InfoLine with your myeloma-related questions and concerns. Phone lines are open 9 a.m. to 4 p.m. (Pacific) Monday through Friday at 1.800.452.CURE in the U.S. and Canada and 1.818.487.7455 worldwide. To submit your query electronically, email [email protected].
(This article was published in the 2024 Summer Edition of the IMF's quarterly publication, Myeloma Today. Read the full publication here.)